Distribution
Distribution is a stage in the pharmacokinetics of a drug in which it move through the blood, and from the blood circulation to the body’s tissues and fluids. Several factors can affect the distribution of an absorbed drug: blood flow, lipid solubility and protein binding. The following text will go into details about each of these factors in the distribution of THC.
THC is a lipophilic compound, meaning that it prefers to be in a “fatty” environment, such as the adipose tissue and the brain. Due to its lipophilicity, THC and its metabolites will rapidly distribute to fatty tissues and highly vascularized organs (organs with lots of blood flow) such as the brain.
1 THC accumulates and is stored in the body’s fat, then slowly released back into the blood.
2 This phenomenon of THC slowly moving back to the blood is called
redistribution.
Pharmacologists can measure drug distribution in humans by
radiolabeling drugs,
analyzing tissue samples from cadavers, and by using indirect analysis techniques, including
non-radioactive imaging techniques.
Blood flow’s effect on distribution
When a drug enters the blood’s circulation, it is delivered throughout the rest of the body. Blood flow plays an important part in how quickly a drug is distributed. Regional blood flow in each organ can influence how and how much of the drug is distributed in those respective organs.
Organs such as the heart, brain, kidney, and liver have a relatively high blood flow.
3 Because of this, drugs distribute faster in these organs. Areas of the body with lower blood flow include adipose tissue (i.e. fat), and skeletal muscle. Drug distribution takes longer in these situations.
3
Blood flow can vary due to a variety of demographic factors. For example, age affects how much of each type of tissue you have. A 25-year old man has a higher percentage of muscle and bone and a lower percentage of fat (adipose) tissue, as opposed to a 75-year old man. Due to this difference, a fat-loving drug of the same dose will have a greater effect in the 25-year-old man as opposed to the 75-year-old man. This is because the 25-year-old will have less fat available for the drug to be bound to, so a greater number of effective compounds will reach the brain and other organs.
4
Drug distribution can be challenging in other areas of the body. Distribution into the fluid around our brains and spine (cerebrospinal fluid), and the central nervous system is made difficult due to the structure of their surrounding cells and blood veins.
3 Drugs also have poor access to the fluid in the ear, the lungs, and around the heart.
3 Another significant obstacle for drug distribution is the blood-brain barrier.
The blood-brain barrier is a border separating blood and brain tissue. The blood-brain barrier keeps out toxic materials and pathogens from the brain, while maintaining constant levels of hormones, nutrients, and water inside the brain. Most drugs face challenges in crossing the blood-brain barrier.
Lipid solubility’s effect on distribution
An important characteristic of a drug that affects its distribution is whether it prefers to dissolve in fats (these drugs are known as fat-soluble), or in water (water-soluble). Fat-soluble drugs usually collect in the fat tissue, while the water-soluble drugs concentrate in the fluid section surrounding the cells. Water-soluble drugs are unable to cross through a cell membrane and fat-soluble drugs can pass through the membrane faster. However, in contrast to water-soluble drugs, fat-soluble compounds cannot easily move through the watery environment of the inside of a cell, and they often need helper-molecules called
transporters to move around. Whenever any of these steps are manipulated by a disease or a medicine, distribution and, thereby, body function can be affected. Besides the cell membranes, fat-soluble medicines can also generally penetrate the blood-brain barrier more easily, while water-soluble drugs cannot. THC is an example of a fat-soluble compound, and indeed can have strong effects on the brain, to which it eventually gets distributed.
5
Protein binding
Plasma is the liquid component of blood, and helps to carry cells, nutrients, waste, and other compounds throughout the body. The proteins in this liquid component are called plasma proteins. When a drug is released into the bloodstream, it can either bind to plasma proteins, or remain unbounded. Protein binding can alter drug distribution, efficacy and concentration.
Only the portion of a drug that remains unbounded can have an effect in the body, get metabolized, and then excreted. The portion of the drug that is bound to these plasma proteins will be inactive.
However, when the unbounded drug leaves the blood and diffuses into tissue, the gradient change causes a portion of the drug that is bound to the proteins to now unbind from the proteins and become free-floating in the blood. The unbounded drugs will now be active and ready to be used by the body.
Albumin, lipoproteins, alpha-1 acid glycoprotein are the plasma proteins that drugs usually bind with. In general, a drug’s acidity or basicity describes what types of chemical reactions the drug prefers to undergo. Albumin usually has an attraction for acidic drugs, while basic drugs bind more to alpha-1 acid glycoproteins and lipoproteins. After drugs leave the bloodstream, they enter tissues and bind to proteins such as receptors.
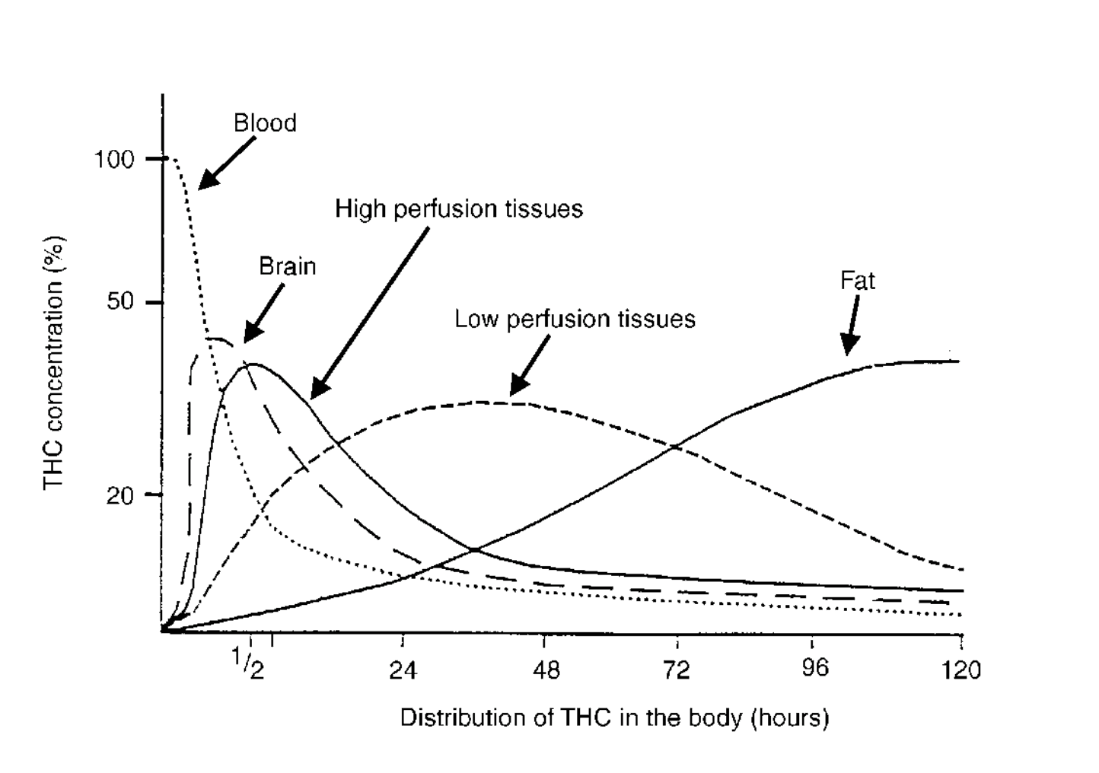 Figure 1: Graph of THC concentrations in different tissues over time, when administered via smoking.5
Figure 1: Graph of THC concentrations in different tissues over time, when administered via smoking.5
In the case of THC, its location in the body changes with time. Looking at Figure 1, for THC administered via smoking, THC is initially entirely in the blood. After roughly 30 minutes, the THC distributes throughout the body, and the brain will have a higher concentration of THC than before. After 120 hours (or exactly 5 days), THC has continued to redistribute, and the body’s fat will now have a higher concentration of THC, while the amounts in the brain and blood have decreased. Figure 2 illustrates this concept. Note that although THC can still be stored, it is no longer active. As time progresses, you see in Figure 1 that the total concentration of THC is no longer at 100% due to excretion.
 Figure 2: Conceptual illustration of the data presented in Figure 1.
Figure 2: Conceptual illustration of the data presented in Figure 1.
Because THC is stored in the body’s fat, THC will stay in the body for a relatively long amount of time compared to other drugs.
THCCOOH (a metabolite of THC) can be detected in urine for over 30 days in chronic/heavy cannabis users.
4
Watch a brief summary video on
cannabis inhalation vs. cannabis ingestion made in collaboration with
Enlighten on
YouTube or on
the screens page.
- Wall, M. E.; Sadler, B. M.; Brine, D.; Taylor, H.; Perez-Reyes, M. (1983). Metabolism, disposition, and kinetics of delta-9-tetrahydrocannabinol in men and women. Clinical pharmacology and therapeutics, 34(3), 352--63.
- Grotenhermen, Franjo (2003). Clinical Pharmacokinetics of Cannabinoids. Journal of Cannabis Therapeutics, 3(1), 3--51.
- Peat, Michael A. (1989). Distribution of delta-9-tetrahydrocannabinol and its metabolites. Advances in analytical toxicology, 2, 186--217.
- Teaching Resource Centre Pharmacology.
- Ashton, C. H. (2001). Pharmacology and effects of cannabis: a brief review. The British journal of psychiatry : the journal of mental science, 178, 101--106.